 Diagnosed and Treated?")
How is ROP diagnosed?
ROP can only be seen with special tools used by an ophthalmologist (of-thuhl-MOL-uh-jist) – a medical doctor who specializes in caring for eyes. The American Academy of Pediatrics (AAP) recommends that all babies who are born earlier than or equal to 30 weeks, weigh less than or equal to 1,500 grams at birth, or have other high-risk factors, receive an ROP eye exam.
A baby’s first ROP exam in the NICU by an ophthalmologist should take place 4 weeks after birth unless they are born earlier than 27 weeks. For babies born earlier than 27 weeks, they will be examined at what would have been the 31st week of the pregnancy. A numbing drop is placed on the eye prior to the procedure to decrease pain. During the exam, the baby will get eye drops to widen their pupils, called dilation. Then, instruments will keep the eye open and in position, so it is easier for the doctor to check all parts of their eyes. The doctor will then use lenses and a headlamp to look inside the eye at the retina so they can see where and how much of the retina may have abnormal vessels (retinopathy).
How serious is my baby’s ROP?
The ophthalmologist will use a few terms to describe a baby’s ROP diagnosis.

LEFT EYE

RIGHT EYE
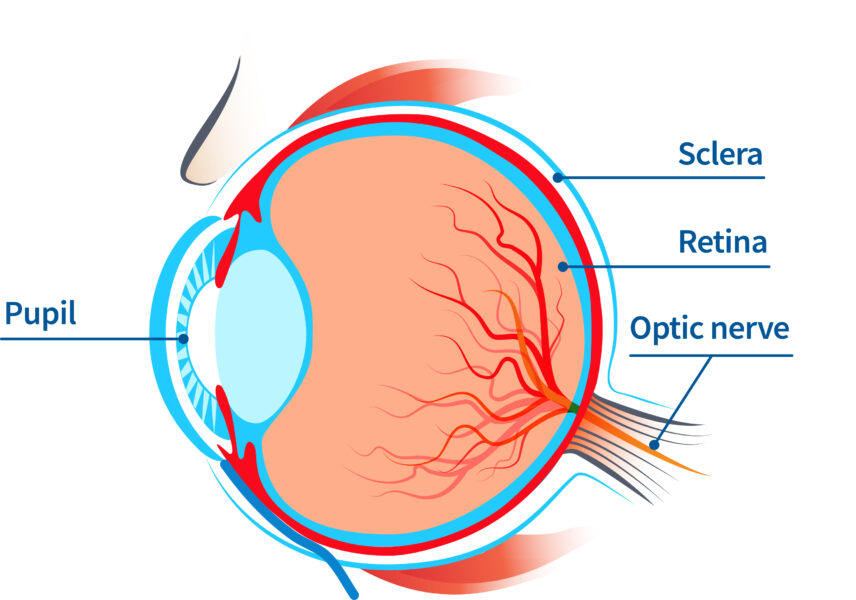
Zone I: A small circular area at the center of the retina and includes the optic nerve. This zone also includes the macula which is the part of the retina that is responsible for central vision and color vision.
Zone II: A circular area around Zone I that includes all the outer part of the retina close to the nose.
Zone III: A half-moon-shaped area that runs along the retina’s outer edge on the side closer to the ear.
The Stage describes how serious ROP is based on the presence and growth of abnormal vessels in the retina. The higher (later) the stage the more serious the disease.
Plus disease describes cases of ROP where the blood vessels around the retina are significantly wider or more twisted than normal.
Pre-plus or plus disease can occur at any stage of ROP and means the baby will require treatment.
What to know about the ROP exam
These eye exams can be uncomfortable for your baby but should only last a few minutes. They are important for protecting their vision and eye health. The dilating eye drops can sometimes make them sensitive to light and more irritable. Nurses at the bedside will monitor your baby closely and create a protective environment, such as turning down lights and providing sugar water, which will help your baby be as comfortable as possible both during and after the examination.
How is ROP treated?
Approximately 10% of ROP cases will be serious enough to require treatment that prevents permanent vision loss or blindness. Your provider will recommend when treatment is needed but is most likely if a child has plus disease or when there is Zone I with Stage 3 ROP or higher.
If ROP progresses to stage 4 or 5, eye surgery may be necessary to prevent the worsening of the retinal detachment.
What follow up is needed for ROP?
All babies with ROP need be checked about every 1-3 weeks until the ophthalmologist determines the ROP has fully resolved and/or the retina has fully grown blood vessels. Then, the baby’s eyes can be checked less often. Some of these checks may happen after the baby goes home from the NICU. It is very important that you keep all scheduled follow-up appointments your doctor recommends. The earlier ROP is identified, the more helpful the treatment will be in preventing vision loss.
Questions to ask the doctor
You are a big part of your child’s care team. Here are some questions that might be helpful to ask when talking with the ophthalmologist:
- What is my child able to see?
- Will my child require medical treatment?
- Does the treatment have any complications?
- What are the chances that my child could go blind from ROP?
- How likely is it that my child’s ROP will return after treatment?
- How frequently do I need to bring my child in for follow-up eye examinations?
- How will my child’s vision be affected in the future?

")
")
 and your child’s lifelong vision health")
 and your child’s lifelong vision health")
 Fact Sheets to Download and Share")
 Fact Sheets to Download and Share")
 Awareness Week")
 Awareness Week")
 Videos")
 Videos")
")
")
This information was developed in partnership with
![]()
![]()
![]()
and made possible with funding from:
![]()
